Welcome to 广东脊祥万岁健康管理有限公司!
Service hotline:
13533607738
18602592233
Welcome to 广东脊祥万岁健康管理有限公司!
Service hotline:
13533607738
18602592233




最新资讯
The small pelvic organs include the colorectum, bladder, urethra, uterus, fallopian tube, ovary and vagina.
The pelvic colon is covered by peritoneum, which connects to the left psoas major muscle midline and sacrum through mesocolon, down to the third sacral vertebra.
The rectum extends downward from the third sacral vertebra to the tip of the coccyx. The anterior and bilateral peritoneum of the upper 1/3 were covered, the anterior 1/3 of the middle 1/3 had peritoneal coverage, and the lower 1/3 had no peritoneal coverage. During pregnancy, the space between the uterus and sigmoid colon becomes smaller, which can lead to or aggravate constipation.

The ureter crosses the front of the common iliac artery into the true pelvis and descends to the pelvic floor along the lateral pelvic wall. At the sciatic spine level, the ureter travels to the front of the vaginal fornix, below the broad ligament, through the uterine artery and the vaginal artery to the side of the vaginal fornix. At this level, the ureter is about 2 cm away from the uterus, where the ureter is vulnerable to injury during hysterectomy. The bladder is located behind the pubic symphysis and in front of the uterus and vagina. The bottom of the bladder is directly connected with the anterior wall of the vagina. The bladder neck is located above the urogenital diaphragm and connects with the urethra. The upper bladder is covered by peritoneum and is in contact with the uterine body and fundus in the anterior flexion position. This layer of peritoneal reflex must be opened during cesarean section. The Retzius space is located between the pubic bone and the bladder and is filled with extraperitoneal adipose tissue. Two sectional anatomical maps on this page show the relationship between the uterus and its surrounding tissues. The upper part of the uterine floor is usually convex and forward. The anterior wall of the uterus is flat and appears to lie forward and down on the bladder. The peritoneum covered in front of the uterus folds over the bladder at the isthmus to form the pit of the bladder uterus. The posterior wall of the uterus is also convex, adjacent to the colon and rectum. The posterior peritoneum covers the uterus and the upper part of the cervix, and then extends the posterior fornix to the rectum to form a rectal uterine depression, or Douglas fossa. The peritoneum forms the anterior and posterior lobes of the broad ligament on the lateral side of the uterus. The cervix is pointed down and posterior to the back wall of the vagina. Only the upper 1/2 of the cervix is covered by peritoneum. The external orifice of the cervix is located at the level of the superior margin of the pubic symphysis, and the coronal plane is located at the level of the sciatic spine.

Pelvic median section
Pelvic viscera and its support system

Pelvic superior view (complete peritoneum)
The intrapelvic fascia (pseudofascia) refers to the fascia that is reversed on the surface of the organs above the pelvic diaphragm. When the hollow organs of the pelvic floor enter the pelvic cavity through the pelvic floor, the fascia of the pelvic cavity attaches to these organs to form a collar-like tubular fibrous tissue upward, which is closely connected with the pelvic floor muscles below. Therefore, three tubular fascial tissues were formed in the pelvic floor, including urethra, bladder, vagina, lower uterus and rectum. The fascial tissue on the surface of these pelvic organs has cross muscle fibers, which can be used to repair the anterior and posterior vaginal wall bulge. It is also in this layer of fascia which covers the lower segment of the uterus. In order to maintain the supporting structure at the top of the vagina, intrafascial hysterectomy is performed in this layer of fascia.
The pelvic fascia on the surface of the bladder, uterus and rectum is connected with the fascia above the pelvic diaphragm, including obturator fascia, iliac fascia and transverse abdominal fascia. The structures that directly or indirectly maintain the position of the uterus include peritoneum, ligaments, fibrous tissues and fibromuscular tissues. The most important of these tissues are the main ligament and the pelvic diaphragm and the pelvic fascia above it.
Bladder-peritoneal reflex and rectal-peritoneal reflex are usually considered anterior and posterior ligaments of the uterus. But they are not real ligaments and have limited support for the uterus. The circular ligament is a flat fibromuscular tissue that travels outward and downward from the anterior wall of the uterus along with the visceral peritoneum and then through the inguinal canal to the labia majoris.

Pelvic superior view
The uterosacral ligament is a true myofibrillary ligament structure, which originates from the upper cervix and travels to the posterior side of the sacrum. The uterine end of the uterosacral ligament fuses with the posterior side of the main ligament and the fascial canal in the pelvic cavity. The broad ligament consists of a wing-like double-folded retrograde peritoneum extending from the lateral wall of the uterus to the pelvic wall. The upper bound of the broad ligament surrounds the fallopian tube and the circular ligament and extends to the upper side to form the pelvic funnel ligament.
Below the broad ligament, the sheathed uterine vessels and the main ligaments are wrapped. There are loose connective tissue, fat, fallopian tube, round ligament, inherent ovarian ligament, parauterine tissue, ovarian crown, paraovarian body, Gartner tube (ovarian crown syndromes), uterus and ovarian blood vessels, lymph and nerve in the two layers of peritoneum of broad ligament. The main ligament or the paracervical transverse ligament (ofMackenrodt) consists of dense fibrous connective tissue and some smooth muscle fibers. The main ligament emanates laterally from the isthmus of the uterus and extends like a tent to the lateral pelvic wall. It is fan-shaped into the obturator and the superior pelvic diaphragm fascia.
This thick fibrous tissue forms a triangular diaphragm with a thick connective tissue sheath enclosing the uterine artery. The main ligament fuses with uterine-vaginal reflex and pelvic fascia and uterosacral ligament posteriorly. Visceral peritoneum and pelvic fascia also support the bladder and rectum.

Anterior pelvic view
lymphatic drainage
The lateral iliac lymph nodes are located above and below the external iliac vessels. They can be divided into two groups: one is located outside the external iliac vessels, the other is located behind the psoas major muscle. The distal end of the posterior lymph nodes was wrapped in the femoral sheath. These lymph nodes receive lymphatic drainage from femoral lymph nodes, external genitalia, deep abdominal wall, uterus and internal iliac artery. Some lymph nodes of the external iliac lymph nodes may flow into the internal iliac lymph nodes, but most of them go up to the common iliac and para-aortic lymph nodes. Most of the lymphatic drainage channels that converge to the extrailiac lymph node come from the vulva, but there are also drainage channels from the cervix and the lower uterus. The external iliac lymph nodes also receive drainage from femoral and internal iliac lymph nodes. The internal iliac lymph nodes are attached to the internal iliac vein. The internal iliac lymph nodes are located in an anatomical triangle with three sides: the external iliac artery, the internal iliac artery and the lateral pelvic wall. The lymph nodes in this area have important clinical significance, including the lymph nodes in femoral canal, obturator lymph nodes and the lymph nodes adjacent to the external iliac vessels. These lymph nodes receive lymph from all organs of the pelvis and from the vulva (including the clitoris and urethra).
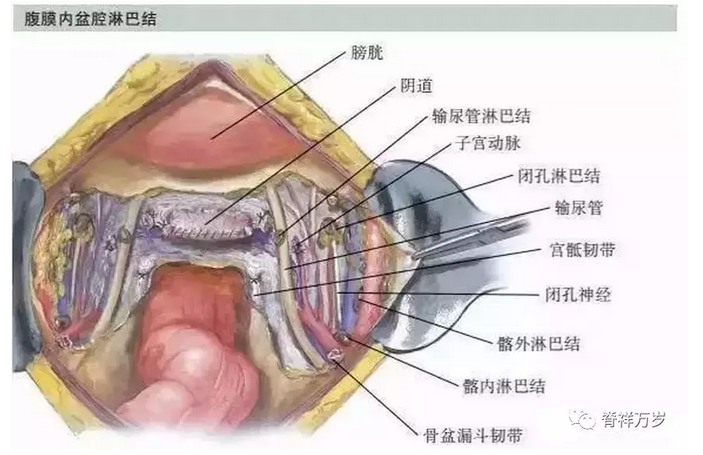
Intraperitoneal pelvic lymph nodes
The number and location of lymph nodes are not fixed, only a considerable number of lymph nodes can be found in the following locations, including the intersection of internal iliac and external iliac vessels, the obturator fossa near obturator vessels and nerves (obturator lymph nodes), and the broad ligament basement adjacent to the cervical ureter running under the uterine artery (ureteral lymph nodes). Sacral median lymph node (promontory)
Lymph nodes) move along the median sacral vessels. The lateral sacral lymph nodes can be found in the sacral cavity and beside the lateral sacral vessels. The internal iliac lymph node receives lymphatic reflux from some blood vessels of the external iliac lymph node, uterus, vagina, bladder, lower rectum, fallopian tube and ovary. Its lymph will flow into the total iliac and para-aortic lymph nodes.
The common iliac lymph nodes are located in the middle and lateral of the common iliac vessels, just below the bifurcation of the aorta. Most of the common iliac lymph nodes are located on the lateral side of the vessels. In addition to draining the lymph in the above lymph nodes, the common iliac lymph nodes also receive lymph from the cervix and upper vagina. In addition, intra-iliac, extrailiac, supra-gluteal and sub-gluteal lymph nodes also flow back into the common iliac lymph nodes. Ilia
The drainage fluid from the total lymph node ascends to the para-aortic lymph node.
The lymph nodes adjacent to the abdominal aorta run in series in front and side of the aorta. These lymph fluids ascend into the lumbar lymphatic trunk and eventually sink into the chylous cistern. Paraaortic lymph nodes receive iliac lymph nodes, abdominal and pelvic organs, ovaries and fallopian tubes, as well as lymph from deep abdominal wall.

Extraperitoneal iliac lymph nodes

Endogenous genital lymphatic drainage
Innervation of internal genitals Pelvic organs are mainly controlled by autonomic nervous system. The sympathetic nerve of the autonomic nervous system originates from the thoracolumbar region of the spinal cord, while the sympathetic ganglion is located near the central nervous system. In contrast, parasympathetic nerves originate from the three sacral segments between the brain nerve and the spinal cord, and their ganglia are located near the visceral organs.


CopyRight © 2017 广东脊祥万岁健康管理有限公司 All Rights Reserved 苏ICP备15053449号-1